Sepsis Huddle
|
Sepsis Huddle (can be initiated by any member of the care team at any time when there is a concern)
|
|||
| Care Area | Emergency Department | Inpatient | PICU |
| Huddle Resources |
|
|
|
| Changes in a patient's clinical status can occur at any time, frequent assessment is indicated | |||
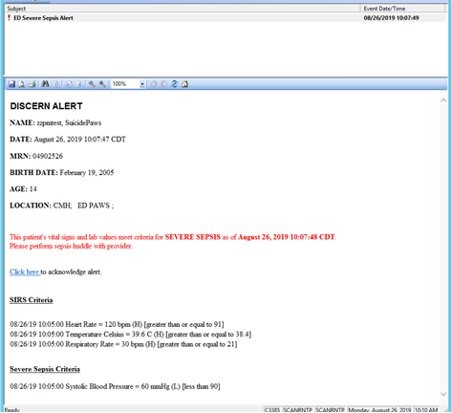 Sepsis Alert-ED RN
Sepsis Alert-ED RN
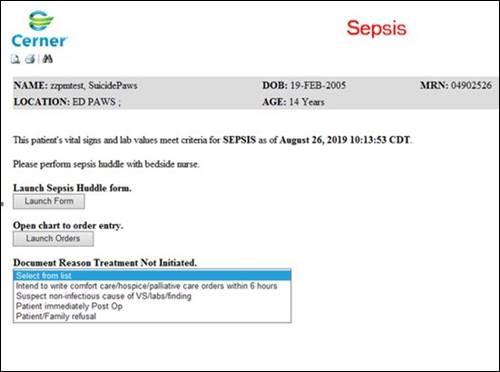 Sepsis Alert-ED Provider
Sepsis Alert-ED Provider
Sepsis Alert-Inpatient RN
Sepsis Alert-Inpatient Provider
For inpatient nurses, there is a Sepsis Secondary Nursing Screen form to complete once an alert is received. The form is scored. If the score is ≥ 2, the inpatient provider is alerted. If the score is < 2, the inpatient provider will NOT receive the alert.
| Proposed Reference Values to Identify Age-Based Vital Sign Abnormalities | ||||
| Age | Tachycardia | Systolic BP | Diastolic BP | Tachypnea |
| (beats per minute) | (mmHg) | (mmHg) | (breaths per minute) | |
| 1 month - 1 year | > 180 | < 75 | < 30 | > 60 |
| > 1 - 5 years | > 140 | < 74 | < 35 | > 40 |
| > 5 - 12 years | > 130 | < 83 | < 45 | > 30 |
| > 12 - 18 years | > 110 | < 90 | < 50 | > 30 |
| Remember, heart rate can be affected by pain, anxiety, medications, and hydration status | ||||
References
Bonfide, C.P., Brady, P.W., Keren, R., Conway, P.H., Marsolo, K., & Daymont, C. (2013). Development of heart and respiratory rate percentile curves for hospitalized children. Pediatrics, 131(4), e1150-1157. https://doi.org/10.1542/peds.2012-2443
Children's Hospital of Philadelphia (2023). Signs and symptoms concerning for sepsis and septic shock. https://www.chop.edu/clinical-pathway/sepsis-emergency-department-inpatient-picu-clinical-pathway
Davis, A.L., Carcillo, J.S., Aneja, R.K., Deymann, A.J., Lin, J.C., Nguyen, T.C., Okuysen-Cawley, R.S., Relvas, M.S., Rozenfeld, R.A., Skippen, P.W., Stojadinovic, B.J., Williams, E.A., Yeh, T.S., Balamuth, F., Brierley, J., de Caen, A.R., Cheifetz, I.M., Choong, K., Conway, E., Jr, Cornell, T., ... Zuckerberg, A.L., (2017). American College of Critical Care Medicine Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock. Critical Care Medicine, 45(6), 1061-1093. https://doi.org/10.1097/CCM.0000000000002425
Gebara, B.M. (2005). Values for systolic blood pressure. Pediatric Critical Care Medicine, 6(4), 500. doi: 10.1097/01.PCC.0000164344.07588.83
Goldstein, B., Giroir, B., & Randolph, A. (2005). International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatric Critical Care Medicine, 6(1), 2-8. https://doi.org/10.1097/01.PCC.0000149131.72248.E6
These pathways do not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the patient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare a pathway for each. Accordingly, these pathways should guide care with the understanding that departures from them may be required at times.