Lyme Disease Testing and Treatment
Consult or refer to Infectious Diseases for guidance or questions
Laboratory Testing
-
For children who present with a classic erythema migrans rash after being in an area where Lyme disease is common, laboratory testing is NOT needed. The diagnosis should be made clinically and the child should be monitored for symptoms of other tickborne illness
-
For children who have symptoms (see clinical syndromes, middle column in the table below) suggestive of Lyme disease without an erythema migrans rash, obtain serologic testing
-
Two-tiered test with enzyme-linked immunosorbent assay [ELISA] or indirect immunofluorescence assay [IFA] for B. burgdorferi antibodies is recommended
-
If either assay yields a positive test result, follow with either a IgM Western immunoblot or a second ELISA test
-
-
For children who have had a positive tick exposure without symptoms suggestive of Lyme disease, laboratory testing is NOT recommended
 Erythema Migrans Rash
Erythema Migrans Rash
Photo courtesy of James Gathany, CDC
Prophylaxis
-
Prophylactic therapy for Lyme disease should only be considered when there is certainty of a high-risk bite (meets conditions below) and the treatment is initiated within 72 hours of tick removal. Otherwise, a wait-and-watch approach is recommended
-
Identified Ixodes spp. vector species -and-
-
Occurred in a highly endemic area (does not include Missouri, Kansas, or any adjacent states [see maps]) -and-
-
The tick was attached for > 36 hours
-
-
Single dose of oral doxycycline 4.4 mg/kg (maximum dose of 200 mg) within 72 hours of tick removal
-
Contact Infectious Diseases if prophylaxis is indicated, but patient is allergic to doxycycline
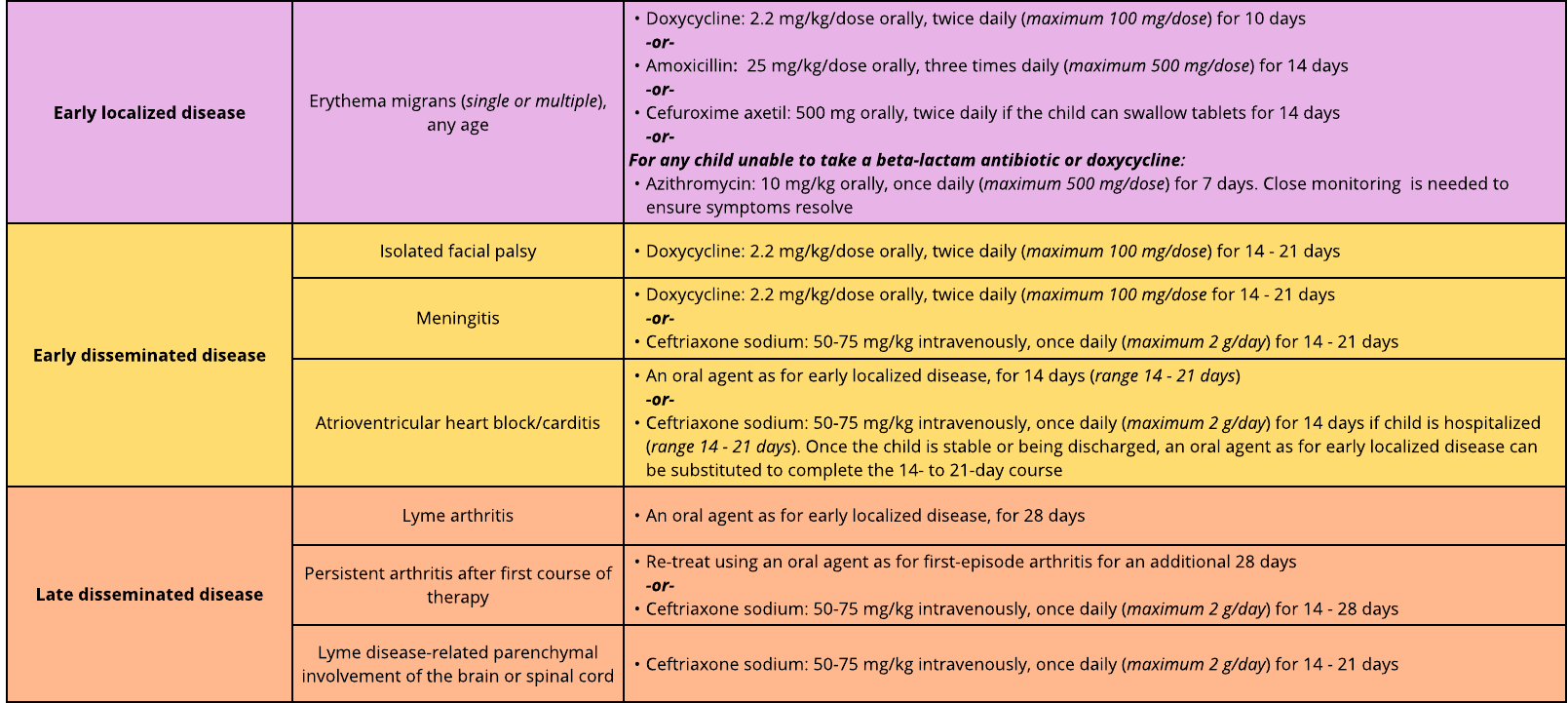
Treatment (based on stage of infection, symptoms, and antimicrobial used)
References
Centers for Disease Control and Prevention. (2007). Erythematous rash [Digital Image]. https://phil.cdc/gov/
Centers for Disease Control and Prevention. (2022). Tickborne diseases of the United States: A reference manual for healthcare providers (6th ed.). U.S. Department of Health and Human Services. https://www.cdc.gov/ticks/hcp/data-research/tickborne-disease-reference-guide/
Committee on Infectious Diseases, American Academy of Pediatrics, Kimberlin, D. W., Banerjee, R., Barnett, E. D., Lynfeld, R., & Sawyer, M. H. (2024). Lyme disease (Lyme Borreliosis, Borrelia burdorferi sensu lacto infection). In Redbook: 2024-2027 Report of the Committee on Infectious Diseases (33rd ed., pp. 549-556). American Academy of Pediatrics. https//doi.org.childrensmercy.idm.oclc.org/10.1542/9781610027373-S3_011006
Lantos, P. M., Rumbaugh, J., Bockenstedt, L. K., Falck-Ytter, Y. T., Aguero-Rosenfeld, M. E., Auwaerter, P. G., Baldwin, K., Bannuru, R. R., Belani, K. K., Bowie, W. R., Branda, J. A., Clifford, D. B., DiMario, F. J., Halperin, J. J., Krause, P. J., Lavergne, V., Liang, M. H., Meissner, H. C., Nigrovic, L. E.,...Zemel, L. S. (2021). Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of Lyme disease. Clinical Infectious Diseases, 72(1), e1-e48. https://doi.org/10.1093/cid/ciaa1215
Pace, E. J., & O'Reilly, M. (2020). Tickborne diseases: Diagnosis and management. American Family Physician, 101(9), 530-540. https://www.aafp.org/afp/2020/0501/p530.html
These pathways do not establish a standard of care to be followed in every case. It is recognized that each case is different, and those individuals involved in providing health care are expected to use their judgment in determining what is in the best interests of the patient based on the circumstances existing at the time. It is impossible to anticipate all possible situations that may exist and to prepare a pathway for each. Accordingly, these pathways should guide care with the understanding that departures from them may be required at times.