Outbreaks, Alerts & Hot Topics: Update on Bird Flu (H5N1)
Column Author & Editor: Chris Day, MD | Director, Transplant Infectious Disease Services; Medical Director, Travel Medicine Program
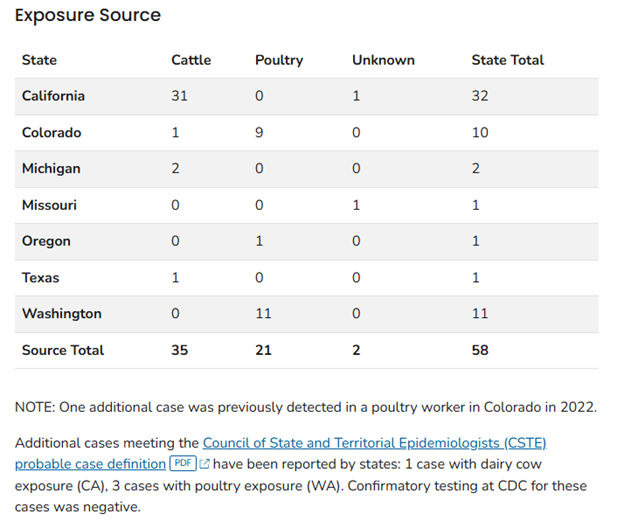
In July of this year, this column provided an update about a developing outbreak of HPAI (highly pathogenic avian influenza) A(H5N1) in cows that resulted in two known human cases of infection. The affected individuals both had contact with cows and both developed conjunctivitis, but otherwise minimal symptoms. Since this report, HPAI A(H5N1) infection has been detected in 58 people, with cattle contacts in 35 cases and poultry contacts noted in 21 cases (see Table). There is no clear origin for infection in two cases, one each in California and Missouri. These latter two cases were detected through national influenza surveillance testing (65,000 other specimens were negative for HPAI A(H5N1)). The remaining positives were detected while monitoring 9,000 people exposed to infected animals and testing more than 470 of these potential cases. Infections in poultry (112 million affected birds) have been noted in 49 states; infections in cows (718 dairy herds) in 15 states.1
Infection with HPAI A(H5N1) should be considered in individuals presenting with either conjunctivitis or an acute respiratory illness within 10 days of a possible exposure. Potential exposures of concern include contacts with sick or dead birds or with livestock or consumption of or contact with raw milk or other unpasteurized dairy products. Spending time in an enclosed space with potentially infected animals or contact with feces or parts (organs, etc.) of infected animals are also potential risk factors. Anyone who is suspicious should contact the state health department to assist in arranging for testing for HPAI A(H5N1). Patients in whom HPAI A(H5N1) is suspected should ideally be placed in an airborne isolation room and, when this is not available, isolated in a private room. They should also, if possible, isolate from their families until testing comes back negative. Health care personnel should use contact and airborne, as well as standard, precautions when evaluating and testing these patients. The Centers for Disease Control and Prevention (CDC) provide details on specimen collection (https://www.cdc.gov/bird-flu/prevention/hpai-interim-recommendations.html). Testing for other viruses, including seasonal influenza and SARS-CoV-2 should also be considered. Treatment with oseltamivir is recommended to be initiated as soon as possible in suspected cases.2
People who are unable to avoid exposure to potential sources of HPAI A(H5N1) for occupational or other reasons should use PPE including an N95 mask or other approved particulate respiratory protection, eye protection, gloves, fluid-resistant coveralls and a disposable head cover. The CDC has provided more detailed guidance to farmworkers, livestock owners, and to other employers whose employees may be at risk. Poultry, eggs and beef should be cooked to safe internal temperatures. Unpasteurized dairy products, including raw milk, have been demonstrated to be contaminated with HPAI A(H5N1). While so far no HPAI A(H5N1) infections appear to have been linked to unpasteurized dairy products, raw milk should be avoided due to potential pathogens including not just HPAI A(H5N1), but also “Campylobacter, E. coli, Listeria, Salmonella, S. aureus, Yersinia enterocolitica, Mycobacterium bovis, Brucella, and Coxiella burnetii.”2,3
The CDC continues to describe the current public health risk of HPAI A(H5N1) as low. The HPAI A(H5N1) case in California involved a child with no clear exposure: family members also reported symptoms but tested negative. There remains no evidence of person-to-person spread in the current outbreak, including in the two cases without clear exposures.4 The pandemic potential of this virus seems to be low, since it may require genetic viral reassortment with a human strain of influenza A or need to undergo significant changes to adapt to humans before human-to-human transmission could reliably occur.5
Currently available seasonal influenza vaccines likely do not provide protection against HPAI A(H5N1) or other potential influenza pandemic viruses but remain important for protection against our current seasonal strains. Some protection against seasonal strains may provide protection against an HPAI A(H5N1)/seasonal influenza co-infection, which could theoretically lead to a reassortment event and a new influenza virus. Therefore, influenza vaccination may be particularly important (especially from a public health standpoint) for workers who are potentially HPAI A(H5N1) exposed. The CDC has developed H5 candidate vaccine viruses, but an effective vaccine for HPAI A(H5N1) is not currently available.6
A vaccine capable of preventing a wide variety of influenza infections, a hoped-for universal influenza vaccine, may be getting closer to reality. One vaccine under development would potentially protect against HPAI A(H5N1). It has been created from a mixture of computationally optimized broadly reactive antigens (COBRA): recombinant proteins from selected influenza hemagglutinins (which include broadly conserved regions of the proteins) that stimulate cross-protective immune responses for multiple strains of H1, H2, H3, H5, H7 and influenza B viruses. This vaccine was formulated as an adjuvanted intranasal vaccine that has been trialed in both mice and ferrets and shows protective immune responses in both animal models. Ferrets were also demonstrated to have protection against severe influenza disease and death when challenged with several strains of influenza. The researchers developing the vaccine are hopeful that clinical trials in humans may begin in the next one to three years.7,8
References:
- H5 bird flu: current situation. Centers for Disease Control and Prevention. Published December 9, 2024. https://www.cdc.gov/bird-flu/situation-summary/
- Highly pathogenic avian influenza A(H5N1) virus: interim recommendations for prevention, monitoring, and public health investigations. Centers for Disease Control and Prevention. Published November 8, 2024. https://www.cdc.gov/bird-flu/prevention/hpai-interim-recommendations.html
- Talking to patients about unpasteurized (raw) milk and highly pathogenic avian influenza. Centers for Disease Control and Prevention. Published June 3, 2024. https://www.cdc.gov/bird-flu/hcp/unpasteurized-raw-milk/index.html
- CDC confirms H5N1 bird flu infection in a child in California. News release. Centers for Disease Control and Prevention; November 22, 2024. https://www.cdc.gov/media/releases/2024/p1122-h5n1-bird-flu.html
- The Lancet Infectious Diseases. What is the pandemic potential of avian influenza A(H5N1)? Lancet Infect Dis. 2024;24(5):437.
- Prevention and antiviral treatment of avian influenza A viruses in people. Centers for Disease Control and Prevention. Published July 19, 2024. https://www.cdc.gov/bird-flu/prevention/index.html
- Uno N, Ebensen T, Guzman CA, Ross TM. Intranasal administration of octavalent next-generation influenza vaccine elicits protective immune responses against seasonal and pre-pandemic viruses. J Virol. 2024;98:e00354-24. doi:10.1128/jvi.00354-24
- Universal flu vaccine candidate protects against infection in mice. News Release. American Society for Microbiology; August 22, 2024. https://asm.org/press-releases/2024/august/universal-flu-vaccine-candidate-protects-against-i
Table. Confirmed human case summary during the 2024 outbreak by state and exposure source. (Source: CDC, reference 1)