Outbreaks, Alerts and Hot Topics: Tularemia Seems to Be on the Rise
Column Author and Editor: Chris Day, MD | Medical Director, Immune Compromised Service & Special Immunology Clinic, Infectious Diseases; Medical Director, International Travel Clinic, Infectious Diseases; Medical Director, Travel Medicine Program
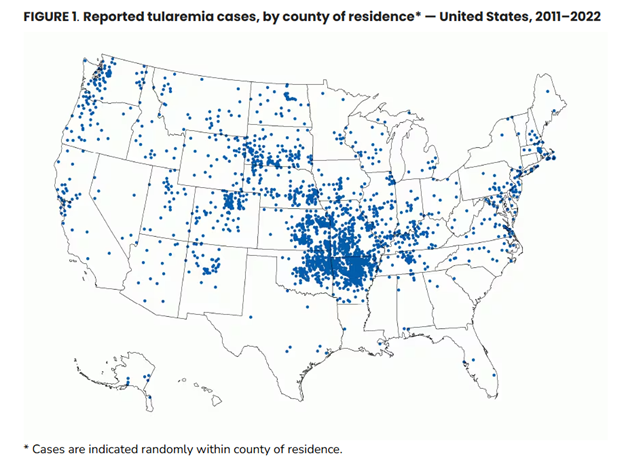
In January 2025, the Centers for Disease Control and Prevention (CDC) issued a report on reported cases of tularemia in the United States from 2011 through 2022, noting an apparent increase in the incidence of infection of 56% from the years 2001 through 2010. Of the 2,462 cases, 50% came from four states: Kansas, Missouri, Arkansas and Oklahoma.
The reason for the increase in reported incidence is unclear. An increase in human cases, or in improved detection, or both, may be responsible. Sixty percent of the cases reported met the surveillance definition of a probable case, compared to only 35% of the cases from 2001 through 2010, with the remainder in both time periods reported as confirmed cases (see Figure 1). The change in the proportions of probable cases may be linked to changes in laboratory testing methods. Previously, most laboratories, including commercial laboratories, used agglutination assays that allowed for comparison of acute and convalescent titers, where a four-fold rise in titers would allow for diagnosis of a confirmed case. Some commercial laboratories are now using newer enzyme-linked immunosorbent assays (ELISAs) that do not allow for easy comparison between titers such that only the definition for a probable case can be met.
Because of the relatively high incidence of tularemia in Kansas and Missouri (0.755 cases/100,000 population in Kansas, 0.383 cases per 100,000 population in Missouri, vs. a national incidence of 0.064/100,000 (see Figure 2: Map, below)), cases of tularemia in our community, including in children, occur at a reasonable frequency. Children aged 5-9 years are one of the highest incidence groups, surpassed primarily by adult males, especially those aged 65-84 years.1,2 Anecdotally, almost all tularemia cases seen in children in our community are presentations of glandular or ulceroglandular tularemia. These infections are recognizable as tender lymphadenitis, often with overlying erythema, that is unresponsive to antibiotics (such as ampicillin-sulbactam or clindamycin) chosen to target Staphylococcus aureus and group A streptococcus. An associated ulcer should lead to earlier consideration of the diagnosis: the ulcer is typically at the site of the bite of a tick, horsefly or other arthropod that was carrying the infection and in the area drained by the affected node. Ulcers on the scalp can be easily missed. Careful inspection of the scalp for children with cervical or occipital lymphadenitis is helpful.
Children with glandular or ulceroglandular tularemia are often hospitalized for indications that include failure of outpatient antibiotic therapy (typically empiric therapy targeted at other organisms), initiation of IV antibiotic therapy, and surgical management of suppurative nodes. They are not typically severely ill. The treatment of choice is IV gentamicin, though ciprofloxacin is sometimes used in mild to moderate cases. Doxycycline is a rarely used alternative. Recurrences of infection do occur despite completion of an appropriate course of treatment, but recurrences may be lower with gentamicin therapy.
Forms of tularemia other than glandular or ulceroglandular are not commonly seen in children in our community. Children using lawn mowers or brush cutters may run over an inhabited rabbit nest and aerosolize tularemia, resulting in pneumonic tularemia, but this possibility seems to be rare. When pneumonic tularemia does occur, it requires immediate reporting to health departments as the organism causing tularemia, Francisella tularensis, is considered to be a potential agent of bioterrorism when acquired by the inhalational route. Several syndromes are associated with ingestion of F. tularensis, and an oculoglandular form of the infection can occur by inoculation of the eye. Overall pediatric mortality is low: only 3 of 199 (1.5%) children died per a review of reported U.S. tularemia cases from 2006 through 2021.3
Diagnosis of tularemia is typically done by serology. Acute titers are frequently negative two weeks or less into illness and titers may need to be repeated after the initial two weeks, looking for either positive titers or a four-fold rise in titers, depending on the laboratory method used. F. tularensis can be cultured in the laboratory but poses a significant risk of inhalation and pneumonic infection for laboratory personnel. The microbiology lab should always be alerted if cultures are submitted on a patient for whom tularemia is in the differential diagnosis.
Figure 1: Tularemia incidence,* by case status† and year — United States, 2011–2022 (Source: CDC, reference 1)
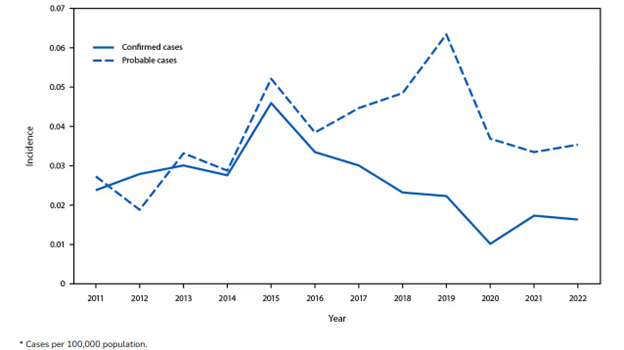
Figure 2: Map (Source: CDC, reference 1)
References:
- Rich SN, Hinckley AF, Earley A, Petersen JM, Mead PS, Kugeler KJ. Tularemia — United States, 2011–2022. MMWR Morb Mortal Wkly Rep. 2025;73:1152-1156. doi:10.15585/mmwr.mm735152a1
- Centers for Disease Control and Prevention (U.S.). Supplementary table. Tularemia — United States, 2011–2022. Published Date January 2, 2025. Series: Morbidity and Mortality Weekly Report (MMWR). https://stacks.cdc.gov/view/cdc/174815
- Wu HJ, Bostic TD, Horiuchi K, Kugeler KJ, Mead PS, Nelson CA. Tularemia clinical manifestations, antimicrobial treatment, and outcomes: an analysis of US Surveillance Data, 2006–2021. Clin Infect Dis. 2024;78 (Supplement 1):S29-S37. doi:10.1093/cid/ciad689