Vaccine Update: Alternative Vaccination Strategies Being Explored for Malaria
Column Author: Yvonne M Carter, MSN, APRN II, FNP-C
Column Editor: Angela L. Myers, MD, MPH | Chief Wellbeing Officer
Could a new vaccine for malaria be in the future? A multi-stage, dose-escalated, double-blind, randomized placebo-controlled trial in the Netherlands suggests an alternative vaccination strategy with the potential to improve protection against infection.
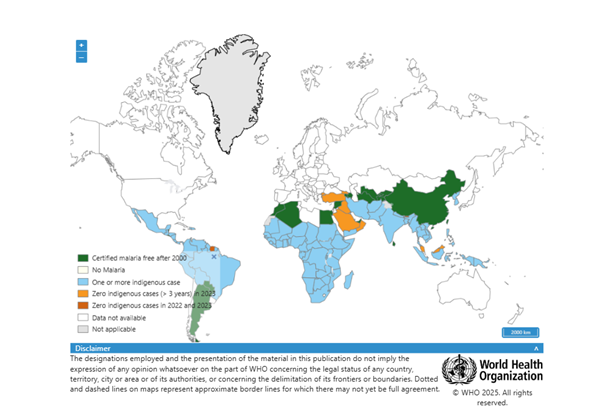
Battling through winter weather in the Midwest makes it difficult to think about anything other than the cold, but spring often brings opportunities to visit warmer climates around the world. Many popular destinations this time of year also come with travel risks, such as exposure to tropical diseases not often seen in the United States. Among these, malaria is often the most pressing concern when traveling to warmer regions close to the equator. While most cases occur in sub-Saharan Africa, it is also prevalent in Central and South America, portions of Oceania, and Southeast Asia (Figure 1). Traditionally, prevention methods for contracting malaria have included drugs such as potent chemoprophylaxis agents or the antibiotic doxycycline that come with tricky dosing schedules and rough side-effect profiles. Researchers in the Netherlands claim that current licensed and available malaria subunit vaccines such as Mosquirix provide only limited, temporary protection against malaria. These vaccines’ mechanisms of action are based on the major sporozoite surface antigen, circumsporozoite protein (CSP), with only 50%-80% protection that lasts approximately one year. A recent study published in the New England Journal of Medicine provides an outlook for a potential vaccine with a reportedly favorable safety profile based on whole, genetically attenuated plasmodium parasites.
Figure 1. Status of Indigenous Malaria Cases
(https://www.who.int/data/gho/data/themes/malaria)
Malaria is spread from one person to another via female Anopheles mosquitoes carrying the parasite Plasmodium falciparum. To spread, the mosquito must bite a human already infected with P. falciparum. In fewer occasions, malaria can spread congenitally, through blood transplant, organ donation or needle-sharing. Once a host is infected, the parasite moves to the liver and replicates within liver cells before moving to the bloodstream to infect red blood cells. Most commonly, malaria may cause flu-like symptoms such as fever, chills, headache, malaise, fatigue, nausea, vomiting and diarrhea. More severe symptoms and potential complications include anemia, jaundice, kidney failure, seizures, mental confusion or coma. Disease may progress to be life-threatening in some instances, if not treated properly. People at highest risk for severe malarial disease include those with little or no recent exposure to malaria parasites (such as travelers or newly relocated vulnerable populations), those heavily exposed to Anopheles mosquito bites, and those living in rural endemic areas with little access to health care. Given that local transmission from person to mosquito to person is extremely rare in the United States, patients and professionals traveling to endemic countries are often at an increased risk of illness.4
In the Netherlands, scientists point toward a second-generation genetically attenuated parasite (GA2) that they report may offer higher protective efficacy against P. falciparum than the previously researched “first generation” early-arresting parasite (GA1). These vaccines work by identifying genes that are essential to the parasite’s intrahepatic development, which allows for production of genetically attenuated malaria parasites that can then be produced and incorporated into vaccine production. GA2 differs from GA1 in that GA1 has short intrahepatic development (24 hours), and GA2 shows complete growth arrest approximately six days post invasion of parasite – later in the liver stage. The recently published GA2 clinical trial was designed to determine whether extended liver-stage antigen exposure can induce better protection than that induced by GA1 (or placebo). Safety and side-effect profiles were also compared.1
The small trial published in the New England Journal of Medicine included a group of 43 adults aged 19-35 years (51% women and 49% men), with 40 subjects completing the trial. In an open-label dose-escalation stage (stage A), 20 adults who had not previously had malaria were randomly assigned to receive either 15 or 50 mosquito bites from mosquitoes infected with GA2. In the double-blind, placebo-controlled phase (stage B), 20 participants were exposed to the bites of 50 mosquitoes in each of three immunization sessions administered at 28-day intervals (nine to GA2, eight to GA1, and three to placebo). Primary end points for both stages included the quantity and severity of adverse events after exposure to GA2, and protective efficacy following infection as measured by (qPCR) assay blood-stage parasitemia greater than 100 P. falciparum parasites per mL after bites from GA2-infected mosquitoes. In stage B, protective efficacy was determined by the number of participants with blood-stage parasitemia after controlled human malaria infection, also measured by qPCR. Results showed that immunization with GA2 resulted in 89% protection (eight of nine participants), versus 13% in the GA1 group (one of eight participants), and 0% (zero of three) in the placebo group.1
Adverse events were similar across the trial groups and were mostly expected. Most common local adverse effects in stage A were erythema and pruritus after mosquito bites (95% and 85% respectively). In stage B, erythema and pruritus were reported by 100% and 96% of participants. Most common systemic adverse events deemed related to trial intervention were myalgia and headache – 20% in stage A and 9% in stage B. Other adverse events included abdominal pain in 40% of stage A participants, malaise and fatigue in 50%, and nausea and vomiting in 60%; however, these events were deemed unrelated to intervention, possibly due to co-occurrence of the COVID-19 pandemic with the timing of the trial. Stage B saw a co-occurrence of COVID-19 across all groups, which may have contributed to reported adverse events as well. The authors note that two participants had elevated levels of troponin T, although the investigator determined these elevations to be unrelated to trial intervention. Elevated liver function tests were seen in another participant but were attributed to antihistamine use.1
Regarding generalizability, authors do note the small sample size (also attributed to the COVID-19 pandemic) and state that more research is needed.1 It is also important to note that while travelers to tropical regions may benefit from this potential vaccine, vulnerable populations such as the immunocompromised or young children in endemic areas such as sub-Saharan Africa are often at the highest risk for complications from malaria. For this reason, more research would be needed in a population more applicable to those the intervention would benefit the most. If this research can be done, the potential for prevention may be great.
In a fast-paced and increasingly digital world, this small study provides an opportunity to reflect on health care professionals’ unique skillsets in clinical judgment (the “art of medicine”) and scientific communication (the “science of medicine”). While interpreting and analyzing research is part of advanced education, and is often part of daily life in academic medicine, translating this information properly to our most applicable and most important population – the patients – can be difficult. For instance, the graphic PDF plain language summary linked in this article is most likely what would be shared with patients. Its conclusion states that the GA2 vaccine offers a higher protective efficacy against P. falciparum than do its predecessors “without known safety concerns.” A patient – or patient’s caregiver – may read this and feel relieved, encouraged or even excited! Yet, we must remember that no drug, vaccine or intervention can ever be without safety concerns. From the most common over-the-counter medications to the most advanced biotechnology, there will always be safety concerns. Our job as a health care community is to communicate with patients and families in a way that empowers them. Trust is placed in health care providers to translate clinical information and advances in medical technology in a way that is in the best interest and wellbeing of the patient. We may consider common adverse effects to be minor, and more serious adverse effects may be deemed unrelated, but that does not necessarily mean that the patient population does not need to know about them. After all, knowledge is power. It is by sharing our knowledge with the wider community – by using both the science and the art of medicine – that we may empower patients and families to make the choices that are best for them.
References:
- Lamers OAC, Franke-Fayard B, Koopman JPR, et al. Safety and efficacy of immunization with a late-liver-stage attenuated malaria parasite. N Engl J Med. 2024;391:1913-1923. doi:10.1056/NEJMoa2313892
- Where malaria occurs. Centers for Disease Control and Prevention. March 18, 2024. Accessed February 11, 2025. https://www.cdc.gov/malaria/data-research/index.html
- Countries with indigenous cases in 2000 and their status by 2023. World Health Organization. Accessed February 10, 2025. https://www.who.int/data/gho/data/themes/malaria
- How malaria spreads. Centers for Disease Control and Protection. Accessed February 11, 2025. https://www.cdc.gov/malaria/causes/